- Special Report
Foreign-Trained Doctors are Critical to Serving Many U.S. Communities
Published
There are more than 247,000 doctors with medical degrees from foreign countries practicing in the United States, making up slightly more than one-quarter of all doctors. Although the data used in this report does not contain information on country of birth or citizenship, evidence from other sources indicates that most foreign-trained doctors are not U.S. citizens—meaning that the majority are foreign-born. These doctors play a key role in providing healthcare for millions of Americans.
This report builds upon other studies that have looked at the critical role foreign-trained doctors play regionally, in underserved communities, in rural areas, and in providing primary health care. It finds that foreign-trained physicians are more likely than U.S.-trained doctors to practice in lower-income and disadvantaged communities and, as a result, their presence is critically important.
More precisely, this report examines foreign-trained doctors in Primary Care Service Areas (PCSAs) and analyzes the socio-demographic characteristics of the populations they serve (see Methodology). For instance, it finds that:
- In areas with the highest poverty rates—where more than 30 percent of the population lives below the federal poverty rate—nearly one-third of all doctors are foreign-trained.
- Where per-capita income is below $15,000 per year, 42.5 percent of all doctors are foreign-trained.
- Where 75 percent or more of the population is non-white, 36.2 percent of the doctors are foreign-trained.
- Where 10 percent or less of the population has a college degree, nearly one-third of all doctors are foreign-trained.
Foreign-trained doctors play such an important role in filling medical shortfalls in disadvantaged communities because of the large disparities in access to healthcare that exist in the United States. Research has found that minorities and the poor are less likely to have health insurance and less likely to have a regular source of medical care. African Americans and low-income Hispanics are more likely than Caucasians and Asians to live in “healthcare deserts”—areas with few or no primary-care physicians. African Americans and Hispanics may be up to twice as likely as whites to live in zip codes with few or no primary-care physicians.
The demand for foreign-trained doctors will only increase as the need for doctors and accessible, affordable healthcare in the United States continues to grow. The Association of American Medical Colleges found that the demand for doctors will continue to outpace supply, leading to a projected shortfall of between 46,100 and 90,400 doctors by 2025, many in primary care. These shortages are compounded by the fact that large numbers of doctors will be retiring in the next few years.
Yet U.S. immigration policies significantly limit the ability of these doctors to immigrate to and practice in the United States. As policy-makers debate what immigration reforms would best serve the national interest, they should keep in mind that foreign-trained doctors are already taking the lead on providing care to many communities across the United States.
Just over one-quarter of doctors in the United States were “foreign-trained” as of 2017, meaning that they received their medical degrees from schools outside of the United States (Table 1). Some of these doctors are U.S. citizens who went abroad for medical school. However, most are not. From 1992 through 2016, 81.3 percent of the 234,850 certifications issued by the Educational Commission for Foreign Medical Graduates (ECFMG) were non-U.S. citizens. (ECFMG issues certifications to International Medical Graduates (IMGs) who have passed the first three components of the United States Medical Licensing Examination, and whose final medical diploma and transcript have been directly verified.)
Table 1: U.S. Physicians by Training Location, 2017
|
|
Number of Practicing U.S. Physicians |
Percentage of Total |
|---|---|---|
|
U.S.-Trained |
727,000 |
74.6 |
|
Trained Abroad |
247,449 |
25.4 |
|
Total U.S. Physicians |
974,449 |
100 |
|
Source: Data from the American Medical Association via DMD Marketing Corporation, February 2017. |
||
The Northeast United States has a considerably higher share of foreign-trained physicians than other regions of the country. In contrast, states in the Western United States have the lowest share: 12 percentage points lower than those in the Northeast (Figure 1). The regional difference is notable since studies have found that some Western states face particularly daunting doctor shortages at the county level. In addition, residents of these counties generally have to travel greater distances for medical care since these western areas are geographically larger.
Figure 1: Foreign-Trained Doctors in the United States, by Region
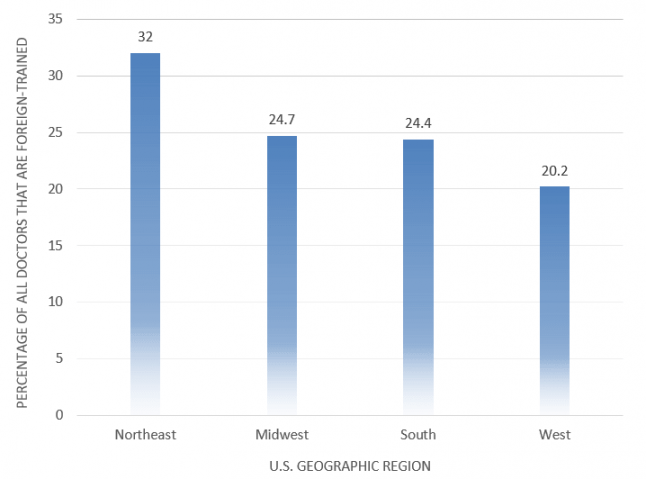
*Regions based on U.S. Census Bureau Regions and Divisions
Source: American Immigration Council analysis of data from the American Medical Association, U.S. Healthcare Resources and Services Administration, 2010 U.S. Census, and 2006-2010 American Community Survey.
The share of doctors who are foreign-trained varies a great deal by medical specialty. Previous studies have reached similar conclusions, finding that foreign-trained doctors are more likely to practice in primary-care fields compared to U.S.-trained doctors, who are more likely to specialize in other areas. For example, the Chicago Council on Global Affairs found that “native-born physicians are choosing more lucrative specializations, such as dermatology, obstetrics, and orthopedics. This leaves generalist positions like family medicine, internal medicine, and pediatrics more likely to be filled by foreign-born practitioners.” This reality is leading to severe shortages of critical primary-care, pediatric, and family medicine physicians in the rural areas of the Midwest and elsewhere.
Experts expect a shortage of both primary-care doctors and specialists to continue in the coming years. By 2025, the American Association of Medical Colleges projects primary care shortfalls ranging from 12,500 to 31,100 doctors, and shortages of non-primary care doctors between 28,200 and 63,700.
Foreign-trained doctors are critical to addressing these shortages, accounting for important shares of primary-care physicians in the United States. Nearly a third (31.8 percent) of all physicians specializing in family medicine, internal medicine, and pediatrics—three specialties associated with primary healthcare—are foreign-trained (Table 2). These 128,099 foreign-trained physicians are among the primary-care doctors recognized by fellow healthcare professionals as “the first line of defense in the healthcare system.” As a result, primary-care physicians deliver most of the country’s preventive and routine services, such as checkups, initial acute-care, and initial diagnoses guiding patients to the appropriate level of care.
Other medical specialties have significant shares of foreign-trained doctors as well. Over half of all geriatric specialists, for example, are foreign-trained, as are nearly 41 percent of all endocrinologists (Table 2). Less than 10 percent of ophthalmologists, emergency room physicians, otolaryngologists, orthopedists, and dermatologists are foreign-trained. The analysis of 27 U.S. physician specialties, shown in Table 2, reveals that at least one-quarter of all doctors in one dozen specialties have been trained outside of the United States.
Table 2: Specializations and Training Locations of Doctors Practicing in the United States
|
Medical Specialty |
Total Physicians in U.S. |
U.S.-trained Physicians |
Foreign-trained Physicians |
U.S.-trained (%) |
Foreign-trained (%) |
|---|---|---|---|---|---|
|
Geriatrics |
6,663 |
3,154 |
3,509 |
47.3 |
52.7 |
|
Endocrinology/Diabetes/Metabolism |
7,613 |
4,500 |
3,113 |
59.1 |
40.9 |
|
Internal Medicine |
197,286 |
121,217 |
6,069 |
61.4 |
38.6 |
|
Medical Genetics |
889 |
578 |
311 |
65.0 |
35.0 |
|
Pathology |
22,530 |
14,691 |
7,839 |
65.2 |
34.8 |
|
Oncology |
18,853 |
12,359 |
6,494 |
65.6 |
34.4 |
|
Cardiology |
33,214 |
21,911 |
11,303 |
66.0 |
34.0 |
|
Neurology |
20,873 |
13,770 |
7,103 |
66.0 |
34.0 |
|
Psychiatry |
52,235 |
35,865 |
16,370 |
68.7 |
31.3 |
|
Other |
40,700 |
29,158 |
11,542 |
71.6 |
28.4 |
|
Pediatrics |
85,854 |
63,124 |
22,730 |
73.5 |
26.5 |
|
Family Medicine |
119,037 |
89,737 |
29,300 |
75.4 |
24.6 |
|
Physical Medicine Rehab |
13,274 |
10,108 |
3,166 |
76.1 |
23.9 |
|
Immunology |
4,914 |
3,759 |
1,155 |
76.5 |
23.5 |
|
Anesthesiology |
50,974 |
39,485 |
11,489 |
77.5 |
22.5 |
|
Surgery |
50,446 |
41,177 |
9,269 |
81.6 |
18.4 |
|
Obstetrics Gynecology |
47,547 |
40,439 |
7,108 |
85.1 |
14.9 |
|
Preventative Medicine |
6,674 |
5,705 |
969 |
85.5 |
14.5 |
|
Neurological Surgery |
6,764 |
5,840 |
924 |
86.3 |
13.7 |
|
Radiology |
46,389 |
40,197 |
6,192 |
86.7 |
13.3 |
|
Urology |
11,513 |
10,137 |
1,376 |
88.0 |
12.0 |
|
Plastic Surgery |
8,393 |
7,394 |
999 |
88.1 |
11.9 |
|
Ophthalmology |
20,337 |
18,718 |
1,619 |
92.0 |
8.0 |
|
Emergency Medicine |
47,432 |
43,801 |
3,631 |
92.3 |
7.7 |
|
Otolaryngology |
11,520 |
10,659 |
861 |
92.5 |
7.5 |
|
Orthopedics |
28,973 |
26,993 |
1,980 |
93.2 |
6.8 |
|
Dermatology |
13,552 |
12,790 |
762 |
94.4 |
5.6 |
|
Total |
974,449 |
727,266 |
247,183 |
74.6 |
25.4 |
|
Source: American Immigration Council analysis of data from the American Medical Association, 2017. |
|||||
It is clear from the available data that foreign-trained doctors are more likely to practice medicine in areas of the United States that have higher shares of poor, less educated, and minority residents. This is notable since research shows that these populations are less likely to have access to health care than in areas with predominantly wealthy, highly educated, and white residents. For example, one study found that, after controlling for other demographic and economic factors, 25.6 percent of African Americans and 24.3 percent of Hispanics lived in zip codes with few or no primary-care physicians, compared to only 13.2 percent of whites.
Analysts often assess healthcare availability at the local level in terms of Primary Care Service Areas (PCSAs). These are collections of zip codes defined by the U.S. Healthcare Resources and Services Administration (HRSA), which provides demographic and socioeconomic information for these geographic areas. The American Medical Association (AMA) provides information on foreign-trained physicians within PCSAs (see Methodology for more detail).
Areas experiencing higher poverty levels have a higher share of foreign-trained doctors. In PCSAs where more than 30 percent of the population lives below the federal poverty line, nearly one-third of all doctors are foreign-trained (Figure 2). Conversely, in areas where 10 percent of the population or less lives below the poverty line, one-quarter of the doctors are foreign-trained.
Figure 2: Foreign-trained Doctors Serving U.S. Population, by Poverty Level
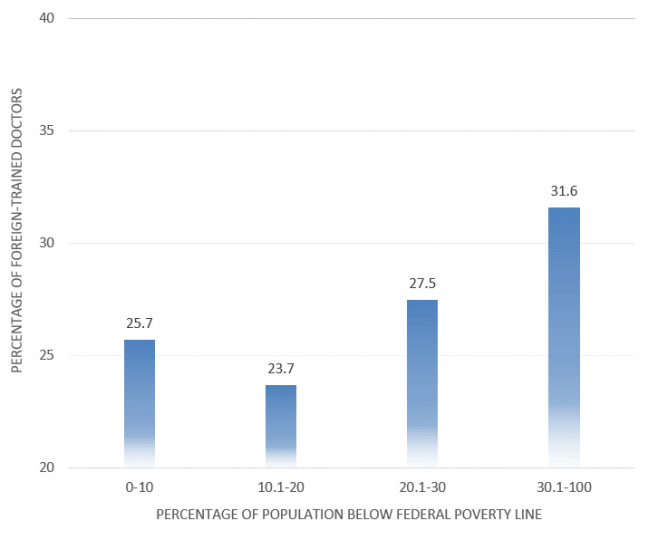
Source: American Immigration Council analysis of data from the American Medical Association, U.S. Healthcare Resources and Services Administration, 2010 U.S. Census, and 2006-2010 American Community Survey.
Foreign-trained physicians have an outsize role in low-income areas. More than half (53.4 percent) of all foreign-trained doctors work in areas where the population has a per-capita income of $30,000 or less. While low per-capita income areas have fewer doctors serving the population overall, significant shares of those doctors are foreign-trained (Table 3). In areas where per-capita income is below $15,000 per year, 42.5 percent of all doctors are foreign-trained. In contrast, in areas where annual per-capita income is more than $50,000, foreign-trained physicians account for 24.1 percent of all doctors.
Table 3: Foreign-trained Doctors Serving U.S. Population, by Per-Capita Income
|
Per-capita Income (USD) |
Total Population |
Number of Doctors per 1,000 Residents |
Total Number of Doctors |
Foreign-trained Doctors | |
|---|---|---|---|---|---|
|
Number |
Percent (%) | ||||
|
$0-15,000 |
8,016,043 |
1.9 |
15,413 |
6,557 |
42.5 |
|
$15,001-20,000 |
45,370,184 |
1.9 |
87,097 |
26,049 |
29.9 |
|
$20,001-30,000 |
162,286,815 |
2.3 |
370,891 |
93,574 |
25.2 |
|
$30,001-40,000 |
58,032,770 |
4.1 |
237,978 |
57,439 |
24.1 |
|
$40,001-50,000 |
18,345,488 |
6.6 |
120,633 |
28,446 |
23.6 |
|
$50,001 or more |
9,370,897 |
10.7 |
100,650 |
24,257 |
24.1 |
|
Source: American Immigration Council analysis of data from the American Medical Association, U.S. Healthcare Resources and Services Administration, 2010 U.S. Census, and 2006-2010 American Community Survey. |
|||||
Consider examples from Ohio and Connecticut, comparing primary care areas with vastly different per-capita incomes (Figure 3). In Youngstown, Ohio, foreign-trained doctors account for 75 percent of the 51 physicians serving 20,690 residents of the state’s fourth PCSA, where per-capita income is $12,141. In contrast, a PCSA in Westport, Connecticut—with a $91,333 per-capita income—has 36,570 residents and 316 doctors, 20 percent of whom are foreign-trained.
Figure 3: Shares of Foreign-trained Doctors in Youngstown, Ohio, and Westport, Connecticut
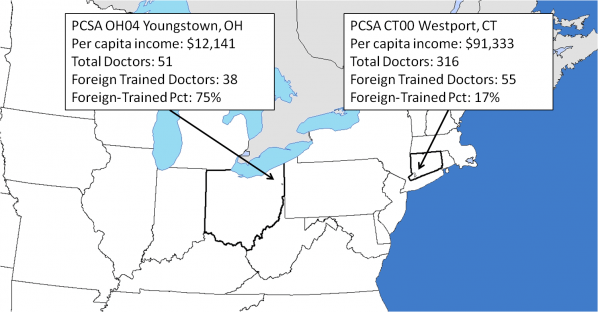
Source: American Immigration Council analysis of data from the American Medical Association, U.S. Healthcare Resources and Services Administration, 2010 U.S. Census, and 2006-2010 American Community Survey.
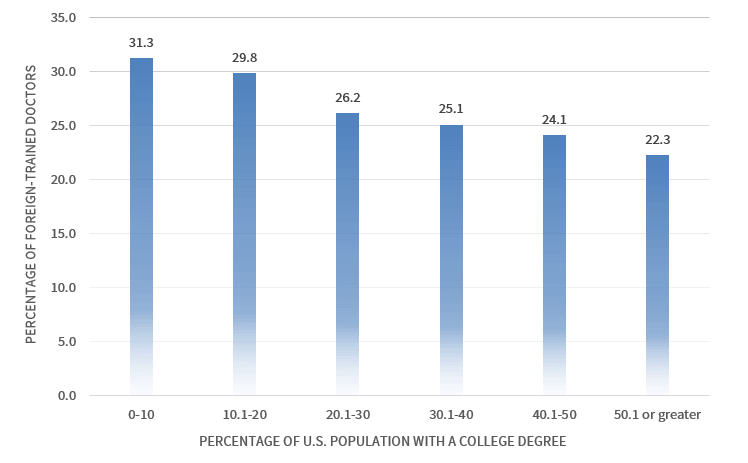
Foreign-trained doctors make up greater shares of all doctors serving populations with lower educational attainment. As shown in Figure 4, the share of doctors who are foreign-trained is higher in areas where few people have college degrees. Where 10 percent or less of the population has a college degree, nearly one-third of all doctors are foreign-trained. Conversely, where more than 50 percent of the population has a college degree, 22 percent of the doctors are foreign-trained.
Figure 4: Foreign-trained Doctors Serving U.S. Population, by Educational Attainment
Source: American Immigration Council analysis of data from the American Medical Association, U.S. Healthcare Resources and Services Administration, 2010 U.S. Census, and 2006-2010 American Community Survey.
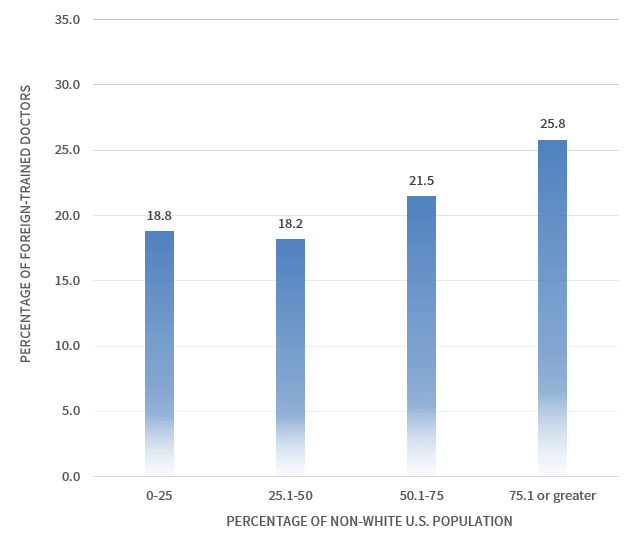
Compared to the number of foreign-trained doctors overall, a significant share serve areas of the United States with greater populations of racial and ethnic minorities. As shown in Figure 5, in areas where 75 percent or more of the population is non-white, 36.2 percent of the doctors are foreign-trained.
Figure 5: Foreign-trained Doctors Serving Non-white Populations in the United States
Source: American Immigration Council analysis of data from the American Medical Association, U.S. Healthcare Resources and Services Administration, 2010 U.S. Census, and 2006-2010 American Community Survey.
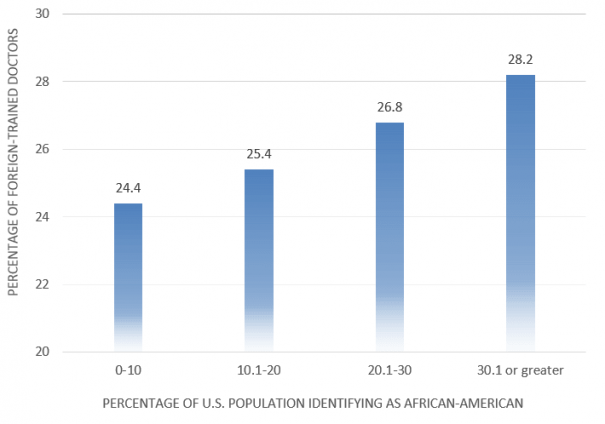
Looking specifically at the African-American population, the share of foreign-trained doctors increases with the share of African Americans living in a PCSA. In areas where African Americans represent between with 0 and 10 percent of the population, 24.4 percent of doctors are foreign-trained, compared to 28.2 percent of doctors in areas where more than 30.1 percent of the population is African American (Figure 6).
Figure 6: Foreign-trained Doctors Serving African-Americans in the United States
Source: American Immigration Council analysis of data from the American Medical Association, U.S. Healthcare Resources and Services Administration, 2010 U.S. Census, and 2006-2010 American Community Survey.
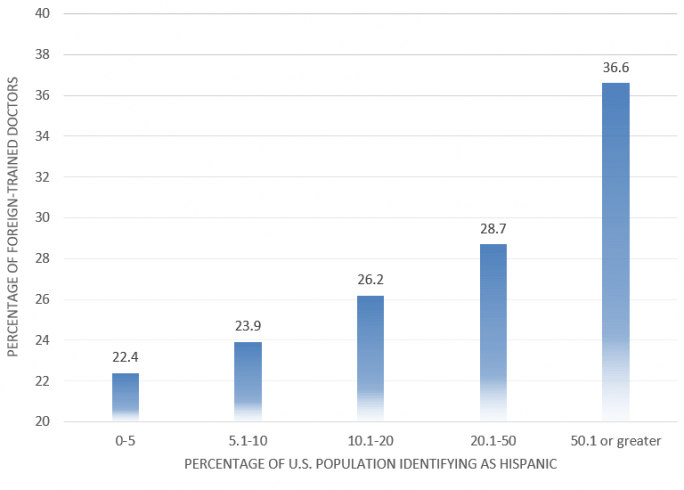
Similarly, the proportion of foreign-trained doctors rises in areas with a greater Hispanic population. As shown in Figure 7, in areas where the Hispanic population is 50 percent or more, 36.6 percent of the doctors are foreign-trained. In contrast, where Hispanics represent less than 10 percent of the area’s population, foreign-trained doctors make up less than one-quarter of all doctors.
Figure 7: Foreign-trained Doctors Serving U.S. Hispanic Populations
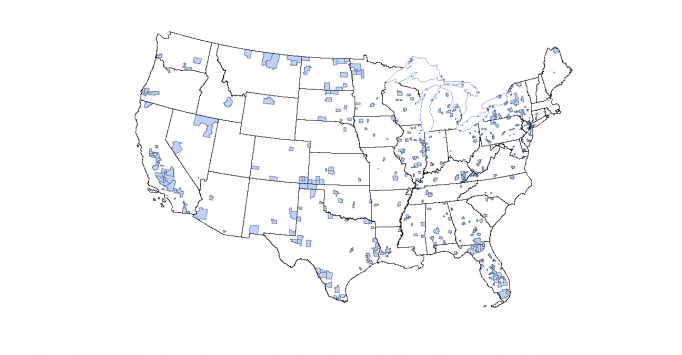
Foreign-trained doctors practice medicine across the United States, yet their impact tends to be most significant in concentrated areas. For example, Florida and California contain large clusters of areas where at least half of the doctors are foreign-trained (Figure 8). Overall, foreign-trained doctors represent at least half of all the doctors, often as primary-care providers, in 553 PCSAs throughout the entire country (Figure 9).
Figure 8: Selected States with Concentrated Areas of Foreign-trained Doctors (at least half)
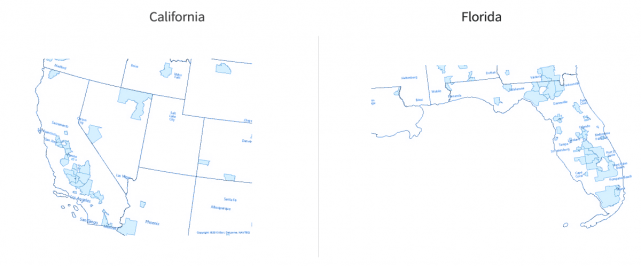
Figure 9: Areas of the United States where at least Half of Doctors Are Foreign-Trained
While the areas where at least half of doctors are foreign-trained make up a small share of all PCSAs in the United States (8.4 percent), the population served is significant and larger than that of areas with no foreign-trained doctors. Combined, 20.8 million people live in areas where foreign-trained doctors account for at least half of all doctors (Table 4). Notably, these areas have greater African-American, Hispanic, and non-White populations than areas with no foreign-trained doctors. People in areas with 50 percent or more foreign-trained doctors depend on these physicians for basic healthcare needs, as nearly 70 percent of primary-care doctors in these locations are foreign trained.
Table 4: U.S. Areas by Share of Foreign-trained Doctors
|
|
Total Population |
Total Number of Doctors |
Number of Foreign-trained Doctors |
|---|---|---|---|
|
PCSAs with No Foreign-trained Doctors |
12,865,657 |
7,108 |
0 |
|
PCSAs with 50 Percent or More Foreign-trained Doctors |
20,847,181 |
45,579 |
26,870 |
|
Source: American Immigration Council analysis of data from the American Medical Association, U.S. Healthcare Resources and Services Administration, 2010 U.S. Census, and 2006-2010 American Community Survey. |
|||
Additionally, the characteristics of these areas can vary significantly and include large, urban areas as well as smaller cities (Table 5). For example, more than half of all doctors in Harrisburg, Pennsylvania; Miami, Florida; and Detroit, Michigan, are foreign-trained.
Table 5: Select Areas with 50 Percent or More Foreign-trained Doctors
|
|
Total Population |
Total Doctors |
Foreign-trained Doctors | |
|---|---|---|---|---|
|
Number |
Percent (%) | |||
|
Bronx, New York (8 combined PCSAs) |
346,902 |
1,506 |
1,188 |
78.9 |
|
Cudahy, Wisconsin |
28,324 |
18 |
11 |
61.1 |
|
Detroit, Michigan* |
198,292 |
2,159 |
1,208 |
56.0 |
|
Harrisburg, Pennsylvania |
19,609 |
63 |
46 |
73.0 |
|
Miami, Florida |
917,619 |
3,729 |
1,988 |
53.3 |
|
Newark, New Jersey** |
190,545 |
717 |
436 |
60.8 |
|
Source: American Immigration Council analysis of data from the American Medical Association, U.S. Healthcare Resources and Services Administration, 2010 U.S. Census, and 2006-2010 American Community Survey. |
||||
* There is only one PCSA labeled “Detroit,” but it does not equal the whole city—i.e., there are far more than 198,292 people in Detroit.
** There are four PCSAs in Newark.
There is a growing need for doctors and accessible healthcare across the United States, especially in underserved areas. As data analyzed in this report show, foreign-trained doctors are critical to meeting that need. Yet U.S. immigration policies significantly limit the ability of these doctors to immigrate to the United States and practice medicine after completing their medical residencies.
Any doctor who wishes to practice medicine in the United States must complete an accredited residency program in the United States or Canada. Foreign nationals seeking to complete this residency in the United States, however, must navigate several additional requirements. First, the Educational Commission on Foreign Medical Graduates (ECFMG) must certify that the foreign national is academically prepared to enter a U.S. graduate medical education program (residency). Then, the physician must “match” into a U.S. residency program, in competition with U.S. medical graduates as well as other international peers.
Exchange Visitor Program and the J-1 Visa
Once accepted into a residency program via the match process, physicians who are foreign nationals must obtain a visa that permits participation in U.S. medical training. Foreign-born medical school graduates commonly apply for a J-1 visa through the U.S. Exchange Visitor Program, which allows ECFMG to sponsor visas for physicians participating in clinical training programs. However, the amount of time clinical trainees can stay in the United States through the Exchange Program is limited generally to seven years, which is the time typically required to complete a residency program and a subsequent fellowship for sub-specialty training.
After completing their residency, J-1 visa holders must generally return to their home countries for two years before they can return to the United States, often on an H-1B (temporary highly skilled nonimmigrant) or L-1 (intracompany transferee) visa. International residency or fellowship graduates who are willing to work in medically underserved areas or with underserved patients for three years can apply for a waiver of the two-year residency requirement. There are several federal agencies that sponsor international physicians for these types of waivers, including the Department of Veterans Affairs, the Department of Health and Human Services, the Appalachian Regional Commission, and the Delta Regional Authority.
The biggest sponsor of J-1 clinical waivers is the “Conrad 30” visa program, which allows each state to recommend up to 30 clinical J-1 waivers annually—though not all states use all of the waivers available to them. Physicians who obtain clinical J-1 waivers may then apply for a temporary H-1B visa in order to legally work in the United States, but must work for the employer sponsoring them for three years. After the three-year period, the physician is eligible to apply for permanent resident status (lawful permanent resident, or LPR, status).
Other Limited Visas Available
There are channels through which foreign medical doctors can train and immigrate to the United States other than the J-1 visa, but they present some obstacles. Doctors may qualify for the temporary H-1B visa classification to complete U.S. residency training, but need a U.S. residency program to sponsor them—something that many programs refuse to do. In addition, to qualify for the H-1B, the physician must generally have passed all three steps of the U.S. medical licensing exam, something that many physicians just beginning residency have not done. The maximum six-year duration of the H-1B can also be problematic for those physicians who wish to complete both residency and fellowship training in the United States, since that training may exhaust almost the entire six years of permissible H-1B time, leaving the physician with no remaining time left in H-1B status to practice medicine following training.
Whether the physician trains in the United States in J-1 status and then obtains a waiver of the two-year home residency requirement, or trains in H-1B status, the path to LPR status following the completion of training is not guaranteed. Doctors may qualify for LPR and thus indefinite work authorization in the United States, but an eligible family member or employer must sponsor them. This process can take multiple years to complete, especially if the physician is from a country that is subject to substantial backlogs, like India.
Foreign-trained doctors play a very important role in providing healthcare to many Americans because of the type of medicine they specialize in and the areas of the country in which they practice. Because they tend to choose primary-care specialties, and because they work in areas of the country with poorer, less-educated, and more minority residents, they are providing important medical services to communities in need.
While U.S.-trained doctors are more likely to choose specializations such as dermatology and orthopedics, foreign-trained doctors fill generalist positions like family medicine, internal medicine, and pediatrics. This means that many Americans’ general and preventative health care needs are filled by doctors who received their training outside of the United States. These findings are important because they show that foreign-trained doctors complement U.S.-trained doctors, filling important healthcare needs and serving underprivileged areas of the country.
As the national conversations over immigration policy and access to healthcare continue, the fact that foreign-trained doctors are taking the lead on providing care to many communities across the United States is an important piece of the puzzle. Policymakers must consider how foreign-trained doctors fill shortages and provide medical care in key areas as they make decisions that may impact doctors’ ability to immigrate to the United States and practice medicine here.
Counts of physicians by zip code of practice location, medical specialty, and location where they earned a medical degree were obtained from the American Medical Association (AMA) via an AMA-approved vendor and are accurate as of February 2017. Characteristics of Primary Care Service Areas (PCSAs) come from the U.S. Healthcare Resources and Services Administration (HRSA). PCSAs can be used to analyze the distribution of health professionals, primary-care services, and access to primary care. A PCSA includes a ZIP code Tabulation Area (ZCTA) with one or more primary care providers, and any additional contiguous ZCTAs whose populations seek the plurality of their primary care from the same providers.
“Foreign-trained physician” in this report refers to individuals who received their medical degrees in a country other than the United States. Foreign-trained doctors include some U.S.-born doctors who received their degrees abroad. Also, U.S.-trained doctors include foreign-born doctors who received their medical education in the United States.
The AMA data on physician counts was reported by ZIP code. The AMA ZIP code data was associated to the PCSAs on the basis of the center of each ZIP code. A ZIP code was assigned to a PCSA when its center (“centroid”) fell within a service area. 95.7 percent of all physicians were successfully associated to a PCSA.
Data on the characteristics of residents of PCSAs was obtained from HRSA. Data from HRSA on the age of populations is derived from the 2010 U.S. Census, while statistics on poverty level, income, and education are from the 2006-2010 American Community Survey. Median and per capita income values are expressed in 2010 U.S. dollars. Racial/ethnic categories such as Black and Latino correspond to U.S. Census Bureau definitions and are self-reported by the population responding to the American Community Survey.
The AMA database counts 976,375 physicians in the U.S., for which 974,449 have information on the location of their training: these 974,449 form the universe of most charts and tables in this report. We were able to assign 932,662 physicians to specific PCSAs; remaining physicians could not be assigned due to slightly differing digitized boundaries in the GIS shapefiles of PCSAs and zip codes.